Objective. The aim of this study was to test the effects on blood pressure of a single bout of low-intensity resistance exercise combined with moderate aerobic walk-based exercise performed by active, controlled hypertensive elderly women.
Method. Forty-two participants were randomized in two types of sessions: exercise session (n = 21), that performed a single bout of combined exercise and control session (n = 21) that keep in rest during the bout. Pre-session, post-session and post-24-hour systolic, diastolic and mean pressure values were evaluated and compared between groups.
Results. Statistical significant reductions were achieved just after the performed bout (7% of reduction) and 24 hours after the bout (9% of reduction) on the diastolic blood pressure values in the exercise session group.
Conclusions. In this population, a single bout of combined session is feasible and safe and has a hypotensive effect on diastolic blood pressure in both immediately and after 24 hours post exercise.
Objetivo. Comprobar el efecto hipotensivo que una sola sesión de ejercicio combinado puede tener sobre la presión arterial de mujeres hipertensas controladas y mayores de 65 años.
Método. Cuarenta y dos participantes fueron asignadas aleatoriamente a dos grupos de sesiones: sesión de entrenamiento (n = 21) que realizó una sola sesión de ejercicios combinados y sesión control (n = 21) que mantuvo reposo durante la misma. Antes, después y tras 24 horas desde la sesión, los valores de presión sistólica, diastólica y medios fueron evaluados y comparados entre grupos.
Resultados. Se encontraron diferencias estadísticamente significativas entre los grupos tras la realización de la sesión (7% de reducción) y tras 24 horas (9% de reducción) en los valores de presión arterial diastólica media del grupo experimental.
Conclusiones. En esta población una sola sesión de ejercicio combinado se propone como aplicable y segura y tiene un efecto hipotensivo en la presión diastólica tanto inmediatamente después como pasadas 24 horas de la intervención.
Introduction
High blood pressure (HBP) has been described as major cardiovascular risk factors that directly cause much of the morbidity and mortality in developed countries1. HBP is a serious public health problem in especially in western-countries2. In Europe, this disease afect the 40% of the population3, reaching the 35% of prevalence in the Spanish population, and, of that, HBP afects the 68% in elderly people aged over 65-years4. It has been estimated that in the year 2025 HBP will have increased by 24% in developed countries and up to 80% in developing ones2.
On the other hand, HBP patients consume the 6% of the medical visits and the 18% of the consultations by chronic affections, being the most common reason to visit primary care physicians5,6. The direct cost associated to the HBP represents in Spain between 2.6 and 3.9 of the global health care total costs7,8. As a result, management of HBP is considered a priority objective in primary and secondary prevention of cardiovascular diseases6 and to promote complementary solutions to help this task has been considered a priority9.
Several studies have been shown that health-related physical fitness (including body composition, flexibility, resistance and cardiorespiratory capacity) is an important predictor of the life expectancy both, in healthy women10 and men11 and in women and men that are affected by a metabolic or osteo-muscular disease12. Furthermore, a good health-related fitness is also a good predictor of the ability to live independently in the elderly population13. On the other hand, the practice of regular physical activity has been shown as a means of prevention and treatment of hypertension14. Despite of the overall benefits that regular physical activity has shown, it is also important to consider the type of population, type of exercise and type of pressure measured when analyzing the effects of the practice of exercise. A recent review of the literature focused on the topic concluded that aerobic physical exercise should be recommended for blood pressure management in controlled hypertensive patients due to its hypotensive effect of this kind of exercise15. On the other hand, althought resistance exercise is an important complement of the aerobic exercise because of its osteomuscular beneficits and its possitive health-related implications16, the use of this kind of exercise in controlled HBP affected patients is under controversy17.
Only two studies had investigated the blood pressure response following a single bout of resistance exercise in controlled HBP patients. Both studies found a decrease in post-exercise and post-12-hour blood pressure values and found that this hypotensive effect was maintained at post-24 hour of the performed exercise18,19. Only one study has determined the effects of combined exercise training recording positive effects on DBP in adults20. However, to our knowledge, no studies have been performed to determine the effects of a single bout of combined aerobic (walk-based) and resistance exercise on the clinic and ambulatory blood pressure in hypertensive elderly women, which might be of interest to obtain the maximum fitness level benefits as well as maintenance and control of the HBP disease. Therefore, the aim of our study was to evaluate the clinical and ambulatory blood pressure values response after performing a single bout of low-intensity resistance exercise combined with moderate aerobic walking-based exercise in HBP-affected elderly women. We hypothesized that in active, hypertensive elderly women, a single bout of low-intensity resistance exercise combined with moderate aerobic walking-based exercise would reach a significant decrease in blood pressure during the recovery period and that this decreased blood pressure would persist for many hours after exercise at least until 24-hour after the performed bout. Even though, post-exercise hypotension might have clinical relevance in hypertensive subjects.
Methods
Experimental protocol consisted of 2 sessions (control and exercise) in which variables were measured before and after interventions. With this protocol, post-exercise values were compared not only with pre-exercise ones but also with the control condition.
Participants
A prospective longitudinal experimental study desing was used. This research was conducted on the premises of an elderly-day center of the south of Spain, under the framework of a social program. Forty-two community-dwelling elderly women affected by HBP (with stable drugs indications) aged between 65 and 75-years participated in the present study. Subjects were contacted through their own organizational structure of the elderly-day center with posters and calls. Furthermore, the participants were verbally and writing informed of the risks, benefits and objectives of the study and signed an informant consent report. Participants were excluded if they had uncontrolled HBP, if they hadn't HBP, and if they had any specific risk to perform the physical exercise required by the experiment. Inclusion criteria were: to be physically active (more than two sessions -maintenance gymnastic comprising walking-based exercise- of 30 minutes per week)21 and medication-controlled HBP over 6 months. The study fully complied with the Declaration of Helsinki for studies on human beings. The study was approved by the Committee on Bioethics and Biosecurity of the University.
Procedures
First, we assessed the anthropometric variables (weight and height) that were used to calculate body mass index. Secondly, the subjects in the study performed a sub maximal test of strength (based on the 10 RM methods)17 and the 40% of the total was estimated, a percentage that was applied during the resistance exercise carried out in the session. The experimental protocol consisted on the performance of two experimental sessions (control and exercise) by all participants, which were conducted in random order with an interval of 5 days between each one (fig. 1). The intensity of the sessions was established as addressed by the American College of Sports Medicine14. Five days before the beginning of the two experimental sessions, all participants in the study carried out two adaptations sessions (carried out on two separate days with 24 hours between each session) in order to ensure the correct execution of the six muscular endurance exercises included in the study. Each exercise of this adaptation was as follow: one set of 10 repetitions at an intensity of 30-40% of 10 RM, one set of 5 reps with 40-60% intensity of 10 RM and one set ranging between three to five reps with an intensity of 60-80% of 10 RM. The rest period was set at one minute between the repetitions and three to five minutes between exercises.
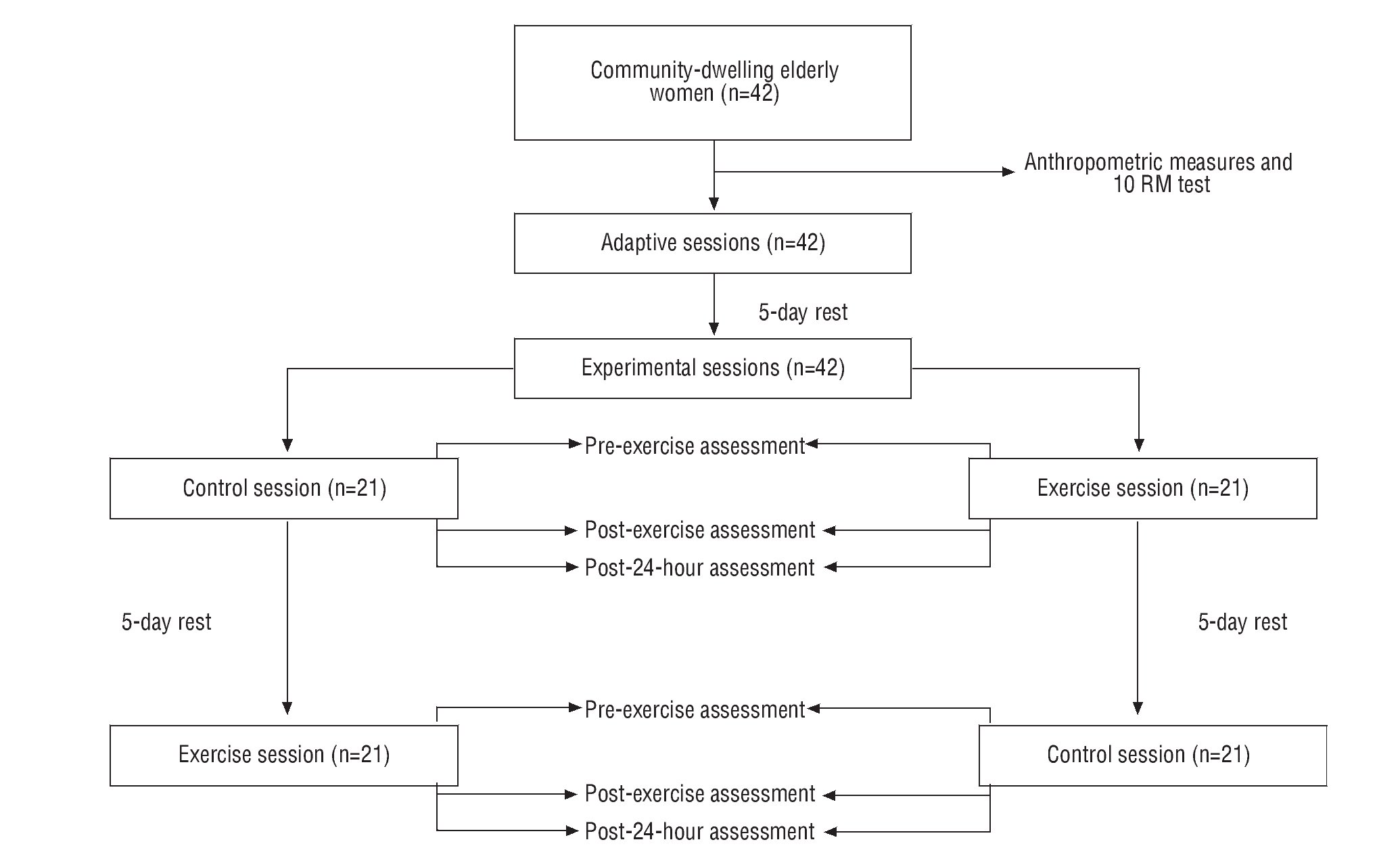
Fig. 1. Experimental protocol schedule.
All participants in the study were asked not to perform any formal physical activity and not to intake alcohol 24 hours before the experimental sessions. Furthermore, participants were asked not to intake caffeine or others substances that could affect blood pressure values. All participants take water before the experiemental sessions but not during it. The experimental sessions was carried out between 9 and 11 am in a thermo regulated room at 21 °C of temperature. In each experimental session the subjects were seated 20 minutes before each intervention. During this period systolic blood pressure, diastolic blood pressure and heart rate were assessed in five minute intervals by auscultation in the dominant arm. The average pre-intervention value was calculated using the average of each of the outlets, excluding the first and last ones. Subsequently, subjects performed the intervention period, which consisted of 45-minute of rest sitting for the control session. The exercise session consisted of performing three sets of 25 repetitions at 40% of 10 RM in six different strength exercises (a variation of bench sitting in a chair squat, biceps, triceps, and shoulder and dorsal opening). A 40 seconds of rest period between series and 90 seconds of rest period between exercises was performed. In order to carry out the resistance exercise conventional low-weight dumbbells (Salter, Barcelona) (0.5 to 5 kg) were used. Then, subjects performed 20 minutes of moderate aerobic exercise based on walking. After the intervention, all participants were asked to rest seated during a 60-minute period. During this period systolic blood pressure, diastolic blood pressure and heart rate were assessed in five minute intervals by auscultation in the dominant arm. The average pre-intervention value was calculated using the average of each of the outlets, excluding the first and last ones. The same method of measurement was used to assess the post 24-hour exercise after the last blood pressure evaluation, asking the subjects that they should not do any exercise and not intake alcohol or other substances that might affect blood pressure values during this period. Both, to assess systolic blood pressure, diastolic blood pressure and heart rate, the auscultation method (Franklin, Argentine) was used22.
Statistical analysis
The different variables were compared at baseline using the Student T test for independent samples, and the distribution of the data was examined by the Kolgomorov-Smirnov test with Lilliefors correction. After confirming that the distribution of all variables was parametric, the comparison between groups of the study variables (systolyc, diastolyc and mean blood pressure values) was performed by a two-way ANOVA for repeated measures adjusted by body mass index and heart rate baseline values. A lineal regression model was performed in order to scan the influence of baseline values on the post-24-hour value in the variables that showed positive statistically significant in the current study. The significance level was set at p<0.05 for all tests performed. All tests were undertaken using SPSS version 18.0.
Results
Forty two elderly hypertensive women were included in the present study. There were no statistically significant differences between sessions at baseline (table 1). Table 2 reveals the comparative effects between sessions on the systolic, diastolic and mean blood pressure. Significant positive effects were found on mean scores registered between the exercise session and control session after the performed bout (7% of reduction; p<0.047) on diastolic blood pressure values and also positive effects were found on the diastolic blood pressure after 24-hour (9% of reduction; p<0.007). In viewing of the performed linear regression model, we found that the baseline value observed in the diastolic blood pressure can explain the 76% the post-24-hour value of the diastolic blood pressure in the subjects of the study (table 3). As we can observe in the figure 2, there exists a tendency to decrease the BP values through the day in all measures after the exercise session. However, we did not find any significant changes after sessions on systolic and mean blood pressures when these values were compared with those from the control session. But we did find a significant decrease in DBP after the experimental session.
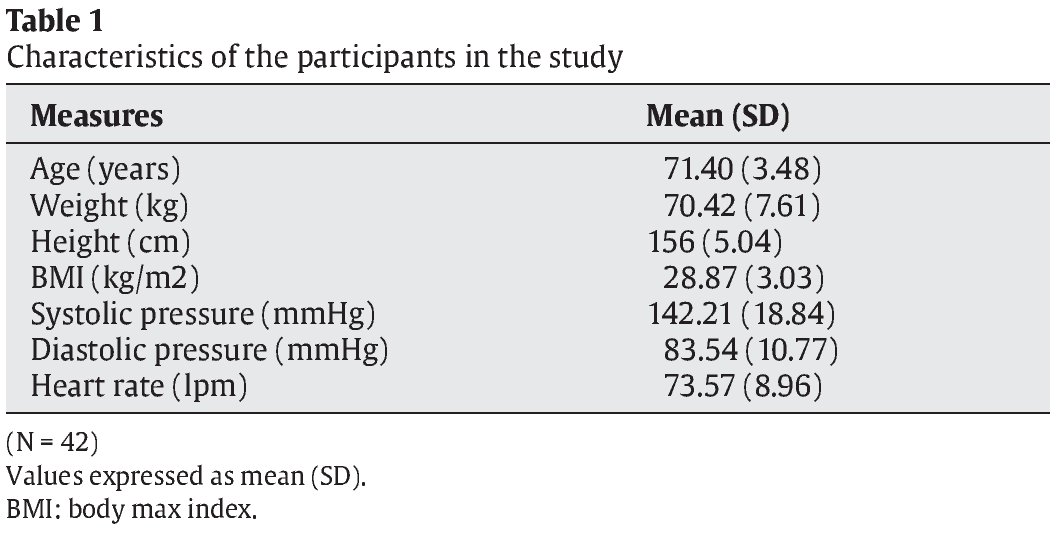
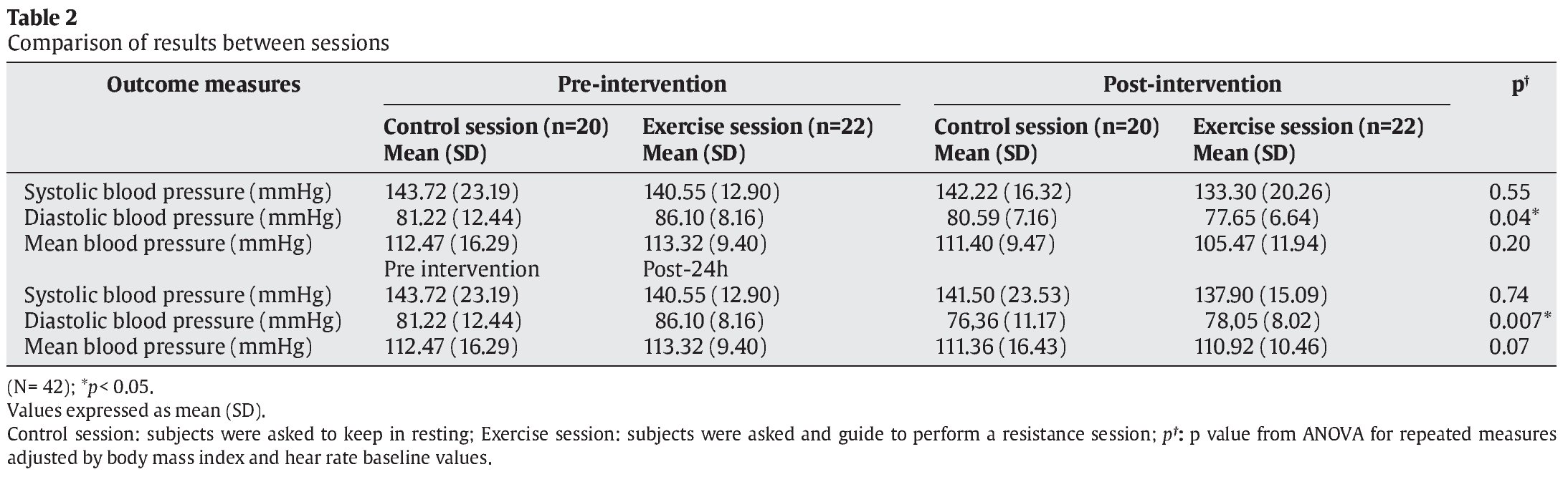


Fig. 2. Blood pressure throughout the different time-points assessment. Data indicates the mean of different blood pressures determined: systolic blood pressure (upper left), diastolic blood pressure (upper right) and mean blood pressure (lower left) in mmHg.
Discussion
Hypotensive effects had been found following aerobic exercise15. Although resistance exercise decreases both, systolic and diastolic blood pressure23, this effect has been very scarcely investigated in hypertensive subjects24,25. On the other hand, resistance training should be proposed as a complement to aerobic exercise due to the musculoskeletal benefits in elderly population26. However, there exist controversial results about the effect of a single bout of resistance on hypertensive subjects15. To our knowledge, there is no scientific evidence showing the effectiveness of a single bout of low-intensity resistance exercise combined with moderate aerobic walk-based exercise on controlled hypertensive patients. As a novelty, we presented the effects of this kind of exercise in over 65-years elderly community-dwelling controlled hypertensive women reporting the blood pressure response values after exercise (clinical value) and at post-24-hour exercise.
The novel finding of our study shows that a single bout of combined resistance and walking-based exercise is feasible, safe and effective significantly decreasing the diastolic blood pressure in both, post-exercise (9%) and after post 24-hour post-exercise (7%). Although the decrease in the diastolic blood pressure found could seem modest, it has been shown that a decrease in blood pressure of at least 2 mmHg is associated with 6% decrease in mortality from stroke and a 4% from coronary heart disease27. In this sense, we could take our results as valuable results in terms of cardiovascular risk prevention.
Auscultatory method is one of the most used method to asses the blood pressure values28. Using this technique, this study found a significant decrease in diastolic blood pressure values after the performed exercise session, while systolic blood pressure values, although showed a tendency of decrease, did not significantly decreased in the exercise session compared with the control session. Although, to date, there is no scientific evidence on the effect of the combination of this type of exercise on the blood pressure values, it is has been shown that a low intensity resistance exercise as well as moderate aerobic exercise produce a hypotensive response in hypertensive patients19,29, which is consistent with our results. Possible explanations could be feasible for these results:
1. As far as we modified the environmental condition of our participants (including a bout of exercise), it has been reported that the trainability of systolic blood pressure values seems partly determined by genetic factors, whereas diastolic blood pressure trainability is more related to environmental effects30. The endothelium is both a target and a mediator of arterial hypertension31, and the reduction of blood pressure reduced by exercise is mediated by improved endothelial function.
2. On the other hand, is well known that physical exercise is associated with the nitric oxide availability in the vascular smooth muscle and endothelium-dependent vasodilatation after a resistance exercise and this effect could decrease the blood pressure values32,33.
3. It has been also accredited that aerobic exercise induces a decrease on the nitric oxide levels and this effect could produce vasodilatation14.
4. Age has been related with different chronic diseases such hypertension34. In addition, it has been reported that age has little or no influence on the changes in the systolic blood pressure35.
5. Furthermore, it has been demonstrated that following a single resistance exercise session and a low-intensity aerobic exercise, diastolic blood pressure decrease more than systolic blood pressure36. As a novelty of this study, post-exercise and post-24h diastolic blood pressure values are greater in subjects with pre-exercise higher values. Thus, in our regression model, we found that the baseline diastolic value can predict the post-24-hour value after exercise in our subjects. According with our data, it has been shown that more severe hypertensive subjects affected could show a major decrease in the blood pressure levels due to the major potential to decrease it17.
Although previous studies have found acute hypotensive effects after a single resistance exercise session, there is controversy about the maintenance of this effect15. Previous studies suggest that a single session of low-intensity resistance exercise produce a hypotensive effect in normotensive subjects, but this response is not maintained over time17. One study conducted in controlled hypertensive women showed a decrease on the blood pressure levels after a single session of resistance exercise that remained after 10 hours19. In contrast, the only study reported in the literature involving untreated hypertensive subjects showed no long term changes, although this study used a high-intensity resistance exercise in their sessions18. On the other hand, it has been proven that a low-intensity aerobic exercise produces a long term hypotensive effect after 24 hours of exercise in controlled hypertensive subjects37. In line with this research, we found that decrease in diastolic blood pressure after a resistance exercise session in combination with moderate aerobic exercise is maintained 24 hours after exercise session. Althrough a large clinical trial is necesary to confirm the long term hypontesive effects of this type of exercise.
Although the scientific literature indicates that there are not chronic changes in blood pressure after a resistance exercise24,25, evidence exists that low to moderate aerobic exercise training has a chronic hypotensive effect in subjects affected by hypertension38. In fact, aerobic exercise is a very powerful tool for the prevention and treatment of high blood pressure disease14. One study reported the beneficial effects of combined exercise in middle adult on reducing the DBP20. This results are in line with our data showing a similar percentage of decrease in our subjects (7% reduction in DBP). Also, although our data did not report significant differences in systolic blood pressure, it could be observed a general tendency to decrease systolic blood pressure values. Thus, this leads us to think that a combined-based training (aerobic and resistance exercise) could cause long-term hypotensive effects in well-controlled hypertensive elderly39.
This study has some limitations. Regarding the sample type, in our study only women were studied so that we could not generalize the obtained results to age-matched men but in agreement with other studies we may think that the blood pressure response could be similar in men than in women35 and, thus, we could apply the combined sessions to both elderly men and women. However more studies are needed to confirm this hypothesis. On the other hand, it was not possible, due to the lack of resources, to assess the ambulatory blood pressure values at other times that we presented in the current study, but our results show a tendency of decrease de blood pressure values at post-24-hour after the exercise bout. Because there is no previous scientific evidence about the effects that the combined aerobic walk-based exercise with low intensity resistance exercise with on blood pressure response, further studies focus in this line of research are necessary to confirm the effects found in our study. Also applied studies are needed in other groups of populations (such elderly over 75 year-old) where the blood pressure values can be expected to be different40. Finally it is necessary to test the effectiveness and cost effectiveness of large longitudinal studies that allow us to decide on the implementation of this kind of therapies as complementary strategies in the health system in addition to the usual care, as a method of public health.
In conclusion, in over 65-year old women affected by controlled high blood pressure, a single bout of combined moderate aerobic walk-based exercise with low-intensity resistance exercise, is feasible and safe and has a hypotensive effect on diastolic blood pressure in both immediately and after 24 hours post exercise, but there is not any effect on systolic blood pressure, which it is maintained both in acute response and after 24 hours of exercise. We could them advice this kind of combined session to improve the properties of both, aerobic moderate walk-based exercise and low-intensity resistance exercise which could have osteo-muscular, metabolic and blood pressure benefices in women elderly population16.
Practical implications
It has been reported that only 32.8% of patients diagnosed with high blood pressure and treated in primary care could control their blood pressure values41. Both, aerobic moderate walk-based exercise and low-intensity resistance exercise are recommended for heart-failed patients but also in normotensive subjects or at the beginning of a resistance training programs where the blood pressure values remains stable over time. By contrast, in hypertensive patients there are many blood pressure fluctuations over the day and therefore the implementation of strategies to help the management and control of such peaks as complementary therapies are necessary. The results of this study suggest that the combination of both types of exercise can reduce and help in the management of the high blood pressure disease, which can help clinicians and professional of exercise in the development of the health promotion programs for this chronic disease.
Conflicts of interest
The authors declare that they have no conflicts of interest.
Acknowledgements
The present study was supported by grants from the Government of Andalusia. Andalusia Center for Development Biology provided human and infrastructure resources. Jesús del Pozo-Cruz was awarded a pre-doctoral fellowship funded by the proyect IMD2010-SC002 from the Andalusia Center of Sport Medicine on behalf of the Government of Andalusia.
History of the article: Received February 1, 2012 Accepted March 18, 2012
Correspondence:
J. del Pozo-Cruz
Departamento de Fisiología, Anatomía y Biología Celular.
Centro Andaluz de Biología del Desarrollo. Universidad Pablo de Olavide-CSIC.
Carretera de Utrera km 1.
41013 Sevilla.
Email:
jdelcru@upo.es